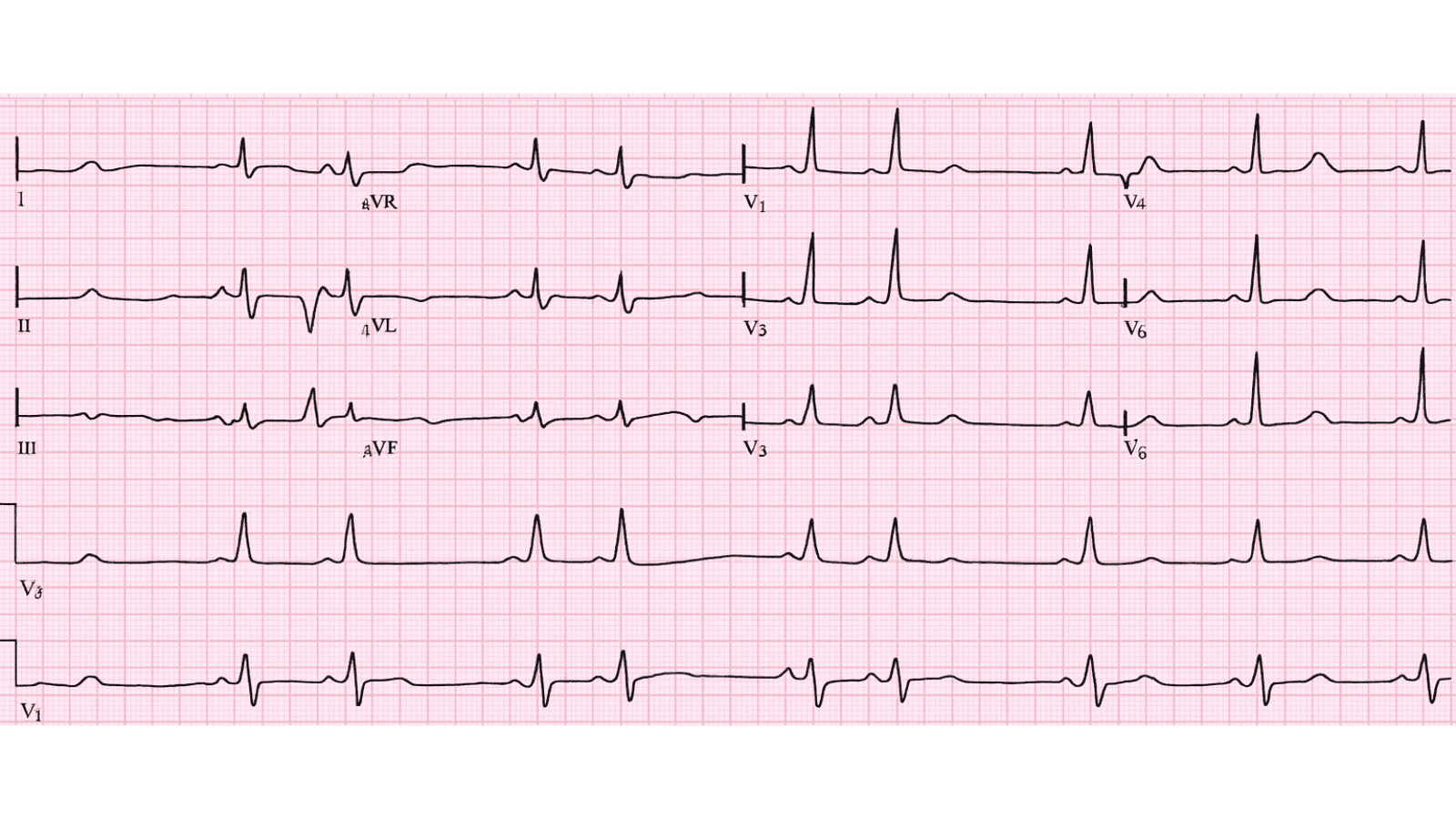
 Second Degree AV Block Mobitz Type II ECG Example Figure 1: Second Degree AV Block Mobitz Type II - Characteristic ECG Pattern
🔑 Key Points at a Glance
- Heart Rate: Variable, often bradycardic
- Primary Significance: Infranodal block, high risk of progression to complete heart block, permanent pacemaker indicated
- Key Management: Temporary pacing if symptomatic, permanent pacemaker placement (Class I indication), avoid AV nodal blocking agents
- Clinical Category: Clinical
Overview and Clinical Significance
Second Degree AV Block Mobitz Type II represents a critical cardiac rhythm pattern that requires immediate recognition and intervention. Infranodal block, high risk of progression to complete heart block, permanent pacemaker indicated
Understanding this ECG finding is essential for emergency physicians, cardiologists, intensivists, and all healthcare providers involved in acute cardiac care. Early recognition and appropriate management can significantly impact patient outcomes and prevent life-threatening complications.
ECG Characteristics and Recognition
📊 Diagnostic ECG Criteria
- Constant PR interval
- Sudden dropped QRS without PR prolongation
- Wide QRS complexes common (infra-Hisian block)
- 2:1, 3:1 or variable block ratio
Systematic ECG Analysis Approach
When analyzing any ECG, including suspected Second Degree AV Block Mobitz Type II, follow this systematic approach:
- Rate: Calculate ventricular rate using the 300-150-100-75-60-50 rule or count QRS complexes in 6 seconds × 10
- Rhythm: Assess regularity by measuring R-R intervals across the entire strip
- P Waves: Identify presence, morphology, and relationship to QRS complexes
- PR Interval: Measure from start of P wave to start of QRS (normal: 0.12-0.20 seconds or 3-5 small squares)
- QRS Complex: Assess duration (normal: Always assess hemodynamic stability FIRST - unstable patients require immediate intervention regardless of the specific ECG diagnosis
Evidence-Based Management
Acute Management Strategy
Primary Treatment Approach: Temporary pacing if symptomatic, permanent pacemaker placement (Class I indication), avoid AV nodal blocking agents
🚨 Emergency Protocol - Time-Critical Actions
- Immediate ABC assessment (Airway, Breathing, Circulation)
- Attach continuous cardiac monitoring and obtain 12-lead ECG
- Establish large-bore IV access (×2) and check bedside glucose
- Administer supplemental oxygen if SpO₂ Recommendations for management of Second Degree AV Block Mobitz Type II are primarily supported by Level A evidence (multiple high-quality randomized controlled trials and meta-analyses).
Summary and Clinical Bottom Line
📋 Clinical Bottom Line
Second Degree AV Block Mobitz Type II is characterized by constant pr interval on ECG. Infranodal block, high risk of progression to complete heart block, permanent pacemaker indicated Primary management: Temporary pacing if symptomatic, permanent pacemaker placement (Class I indication), avoid AV nodal blocking agents Key takeaway: This is a life-threatening emergency requiring immediate recognition and treatment - time-critical intervention saves lives
About the Author
Dr. Raj K
Emergency Medicine Physician Dr. Raj K is a board-certified Emergency Medicine physician with extensive experience in acute cardiac emergencies, advanced ECG interpretation, and critical care. He is passionate about medical education and bringing evidence-based emergency medicine knowledge to healthcare providers worldwide through E-PulsePoints. His clinical expertise includes STEMI management, complex arrhythmia recognition, and emergency cardiac procedures.